M
myopybyproxy
flickerbeat \\ gibberish-noise
- Dec 18, 2021
- 864
What dose should be taken if using quetiapine as a sedative? I've seen varying conflicting information - albeit, from the perspective of 'what side effects did you get from your dose' - ranging from 25mg to over a gram. The thread regarding SN - which I am not using, only read up on it to gather as much information as possible - mentions specific dose ranges engage different receptors and mechanisms of action, which I don't understand, but that's aside from the point. I've got 50mg dimenhydrinate (H1 antagonist) as my antiemetic, which I will take orally approximately 35 minutes prior to my last act. But I'm IVing anyhow so vomiting should not be a concern. If I am wrong please correct me on this.
I am taking 80 proof ethanol, some alprazolam and clonazepam - I am sure the benzos are mostly fake, if you are wondering why I bother with quetiapine at all given the rest of my list - some potentiators (full list of potential and currently planned substances in this thread), and oxycodone - ibid - orally approximately 10 minutes prior to the injection. From previous experience dabbling with benzos, they tend to onset quickly, and I don't want to just fall asleep. Or worse, alert someone whilst blacked out and wake up in hospital once again. That is not one experience I would like to repeat.
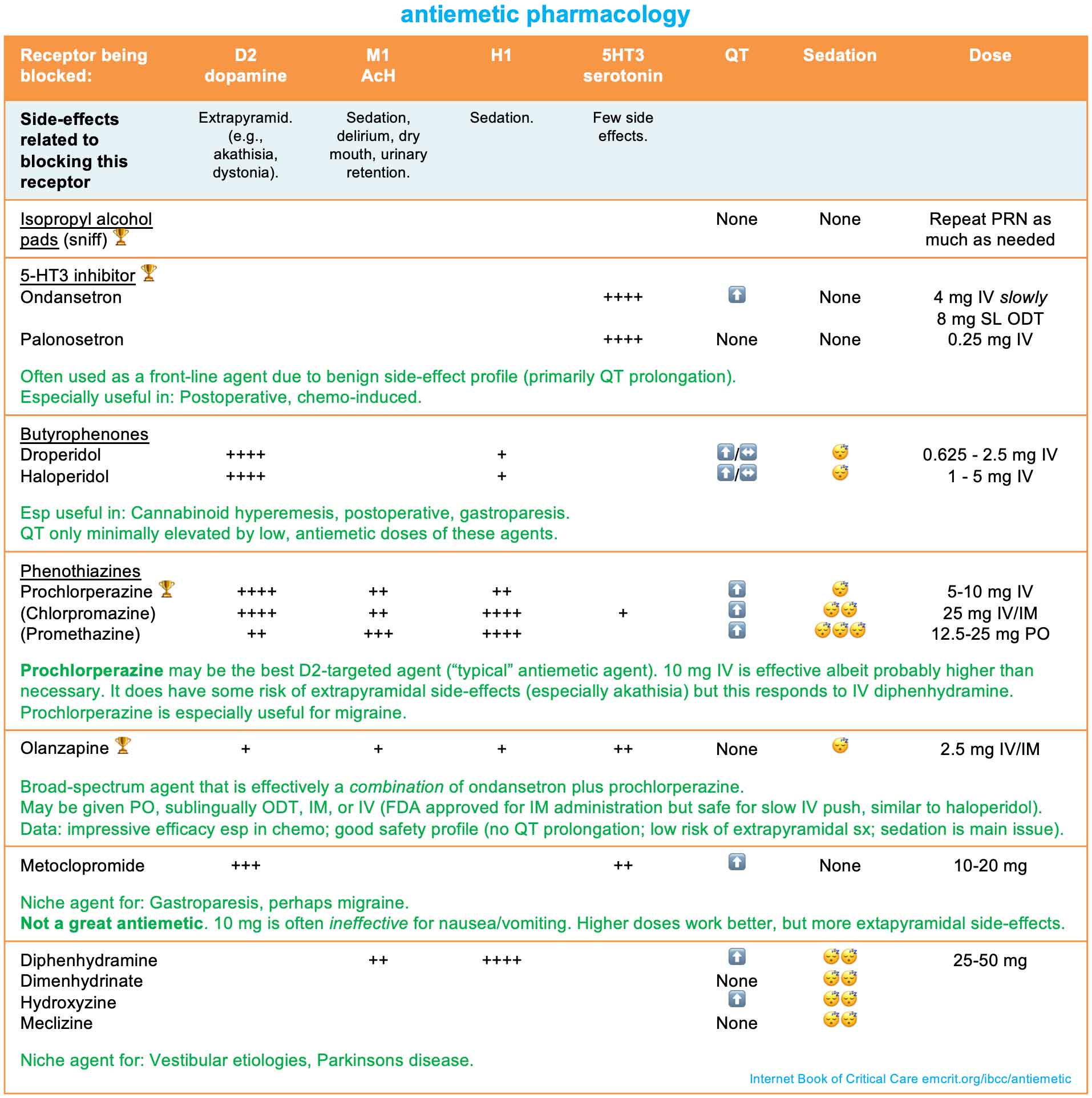
What is the mechanism by which nausea occurs when taking opiates and alcohol - serotonin, H1/2, D2, etc? Is that mechanism dose dependent or is the property the same regardless, as with SN? I have not been able to find this information online. From the aforementioned SN resource thread, 50mg quetiapine seems to have the same antiemetic mechanism as dimenhydrinate via H1 antagonism, whereas 100mg and 300mg antagonises serotonin (5HT) and D2 receptors, respectively.
I notice a 50mg dimenhydrinate will alleviate weekend-drinking-induced nausea, but this is - although with some potentiators that I plan to use in my method - without the other substances such as quetiapine, opiates, benzos etc. And I have never tested the dimenhydrinate effectiveness when drinking amounts which will give me alcohol poisoning - assuming I don't vomit most of the alcohol before it is absorbed. So perhaps my singular tiny pill will be useless overall. I don't know. Input is welcome.
Furthermore, how far in advance should the quetiapine be taken - assume titration during the weeks leading up to expiry date - specifically the last dose once steady-state blood levels have been reached with the titration? That is, how long will it take for the effects to hit? I am not asking about peak plasma concentrations. Rather, I would like to know at what point the sedative effects begin to impair functioning, ie carrying out the rest of the method. Again, preliminary browsing of anecdotal experiences suggest a range from immediately to ninety minutes. This seems to be dose dependent as well.
If anyone could chime in on this, I would be much appreciative. Subjective anecdotal experience welcome as well as research articles. Any information, please - include as much numerical information as possible in your post - particularly the quetiapine dose and how long it took for sedation to occur.
I know this has been a long post. Thank you for reading the whole of it, if you did. I wanted to give the full background so those giving advice would be able to take it into consideration. In synopsis, my questions:
--> What dose will render quetiapine an efficient sedative?
--> How many minutes before such dose is ingested until sedation occurs?
--> Is opiate and alcohol nausea due to serotonin, dopamine, histamine, or some other mechanism?
I am taking 80 proof ethanol, some alprazolam and clonazepam - I am sure the benzos are mostly fake, if you are wondering why I bother with quetiapine at all given the rest of my list - some potentiators (full list of potential and currently planned substances in this thread), and oxycodone - ibid - orally approximately 10 minutes prior to the injection. From previous experience dabbling with benzos, they tend to onset quickly, and I don't want to just fall asleep. Or worse, alert someone whilst blacked out and wake up in hospital once again. That is not one experience I would like to repeat.
What is the mechanism by which nausea occurs when taking opiates and alcohol - serotonin, H1/2, D2, etc? Is that mechanism dose dependent or is the property the same regardless, as with SN? I have not been able to find this information online. From the aforementioned SN resource thread, 50mg quetiapine seems to have the same antiemetic mechanism as dimenhydrinate via H1 antagonism, whereas 100mg and 300mg antagonises serotonin (5HT) and D2 receptors, respectively.
I notice a 50mg dimenhydrinate will alleviate weekend-drinking-induced nausea, but this is - although with some potentiators that I plan to use in my method - without the other substances such as quetiapine, opiates, benzos etc. And I have never tested the dimenhydrinate effectiveness when drinking amounts which will give me alcohol poisoning - assuming I don't vomit most of the alcohol before it is absorbed. So perhaps my singular tiny pill will be useless overall. I don't know. Input is welcome.
Furthermore, how far in advance should the quetiapine be taken - assume titration during the weeks leading up to expiry date - specifically the last dose once steady-state blood levels have been reached with the titration? That is, how long will it take for the effects to hit? I am not asking about peak plasma concentrations. Rather, I would like to know at what point the sedative effects begin to impair functioning, ie carrying out the rest of the method. Again, preliminary browsing of anecdotal experiences suggest a range from immediately to ninety minutes. This seems to be dose dependent as well.
If anyone could chime in on this, I would be much appreciative. Subjective anecdotal experience welcome as well as research articles. Any information, please - include as much numerical information as possible in your post - particularly the quetiapine dose and how long it took for sedation to occur.
I know this has been a long post. Thank you for reading the whole of it, if you did. I wanted to give the full background so those giving advice would be able to take it into consideration. In synopsis, my questions:
--> What dose will render quetiapine an efficient sedative?
--> How many minutes before such dose is ingested until sedation occurs?
--> Is opiate and alcohol nausea due to serotonin, dopamine, histamine, or some other mechanism?